Current issue
Accepted manuscript
About the Journal
Scientific Council
Editorial Board
Regulatory and archival policy
Code of publishing ethics
Publisher
Information about the processing of personal data in relation to cookies and newsletter subscription
Archive
For Authors
For Reviewers
Contact
Reviewers
Annals reviewers in 2025
Annals reviewers in 2024
Annals reviewers in 2023
Annals reviewers in 2022
Annals reviewers in 2021
Annals reviewers in 2020
Annals reviewers in 2019
Annals reviewers in 2018
Annals reviewers in 2017
Annals reviewers in 2016
Annals reviewers in 2015
Annals reviewers in 2014
Annals reviewers in 2013
Annals reviewers in 2012
Links
Sklep Wydawnictwa SUM
Biblioteka Główna SUM
Śląski Uniwersytet Medyczny w Katowicach
Privacy policy
Accessibility statement
Reviewers
Annals reviewers in 2025
Annals reviewers in 2024
Annals reviewers in 2023
Annals reviewers in 2022
Annals reviewers in 2021
Annals reviewers in 2020
Annals reviewers in 2019
Annals reviewers in 2018
Annals reviewers in 2017
Annals reviewers in 2016
Annals reviewers in 2015
Annals reviewers in 2014
Annals reviewers in 2013
Annals reviewers in 2012

Long-term, complex orthodontic treatment of patient with Apert syndrome – from severe malocclusion to functional and aesthetic result
1
University Dental Centre of Medical University of Silesia, Katowice, Poland
Corresponding author
Ann. Acad. Med. Siles. 2025;79:139-145

KEYWORDS
TOPICS
ABSTRACT
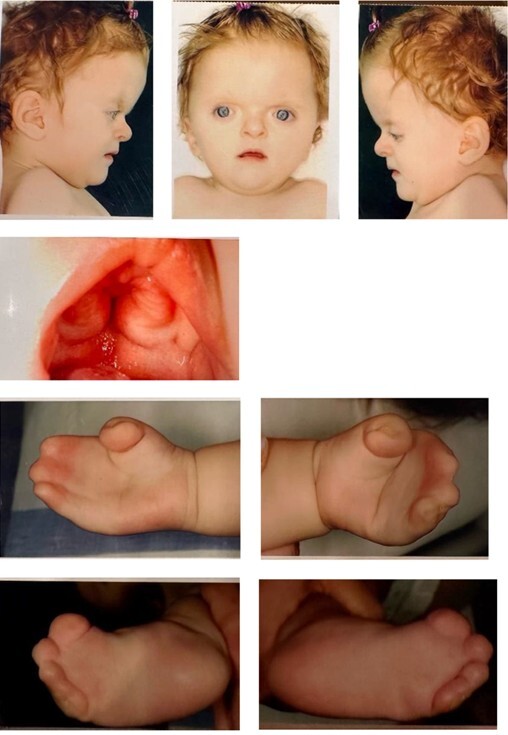
This case report describes the orthodontic treatment of a 2-year-old female with Apert syndrome, initially admitted to the Clinic of Congenital Abnormalities in the University Dental Centre of Medical University of Silesia in Katowice in 2004. Following craniofacial surgery for premature skull fusion, the patient exhibited characteristic Apert syndrome features, including premature fusion of skull bones, midfacial hypoplasia, and syndactyly. Removable appliances were used between 2007 and 2013 to manage dental development and teeth loss, followed by craniofacial osteoplasty in 2013–2014 to correct significant maxillary underdevelopment. Fixed orthodontic treatment was initiated in December 2014, focusing on aligning teeth, correcting malocclusion, expanding the upper arch, and managing crowding. Despite treatment challenges, such as poor oral hygiene the 6-year orthodontic treatment yielded a satisfactory functional and aesthetic outcome. The patient achieved correct overjet and overbite, reduced crowding, and improved jaw relations, though some occlusal problems, including a residual posterior crossbite and minor crowding, persisted. Almost 4-year follow-up demonstrated stable results, although bruxism was developed, requiring a nightly splint. Continued follow-up is essential for managing long-term stability in this complex case.
REFERENCES (20)
1.
Cohen M.M. Jr, Kreiborg S. A clinical study of the craniofacial features in Apert syndrome. Int. J. Oral Maxillofac. Surg. 1996; 25(1): 45–53, doi: 10.1016/s0901-5027(96)80011-7.
2.
Wilkie A.O., Slaney S.F., Oldridge M., Poole M.D., Ashworth G.J., Hockley A.D. et al. Apert syndrome results from localized mutations of FGFR2 and is allelic with Crouzon syndrome. Nat. Genet. 1995; 9(2): 165–172, doi: 10.1038/ng0295-165.
3.
Slaney S.F., Oldridge M., Hurst J.A., Morriss-Kay G.M., Hall C.M., Poole M.D. et al. Differential effects of FGFR2 mutations on syndactyly and cleft palate in Apert syndrome. Am. J. Hum. Genet. 1996; 58(5): 923–932.
4.
Munarriz P.M., Pascual B., Castaño-Leon A.M., García-Recuero I., Redondo M., de Aragón A.M. et al. Apert syndrome: Cranial procedures and brain malformations in a series of patients. Surg. Neurol. Int. 2020; 11: 361, doi: 10.25259/SNI_413_2020.
5.
Kahnberg K.E., Hagberg C. Orthognathic surgery in patients with craniofacial syndrome. I. A 5-year overview of combined orthodontic and surgical correction. J. Plast. Surg. Hand Surg. 2010; 44(6): 282–288, doi: 10.3109/2000656X.2010.516594.
6.
Carpentier S., Schoenaers J., Carels C., Verdonck A. Cranio-maxillofacial, orthodontic and dental treatment in three patients with Apert syndrome. Eur. Arch. Paediatr. Dent. 2014; 15(4): 281–289, doi: 10.1007/s40368-013-0105-9.
7.
Fearon J.A., Podner C. Apert syndrome: evaluation of a treatment algorithm. Plast. Reconstr. Surg. 2013; 131(1): 132–142, doi: 10.1097/PRS.0b013e3182729f42.
8.
Verdonck A., Bertrand J., Carels C., Swinnen S., Schoenaers J. Orthodontic and orthognathic management of a patient with Apert syndrome: a case report. J. Orthod. 2010; 37(2): 121–127, doi: 10.1179/14653121042984.
9.
Breik O., Mahindu A., Moore M.H., Molloy C.J., Santoreneos S., David D.J. Apert syndrome: Surgical outcomes and perspectives. J. Craniomaxillofac. Surg. 2016; 44(9): 1238–1245, doi: 10.1016/j.jcms.2016.06.001.
10.
Fadda M.T., Ierardo G., Ladniak B., Di Giorgio G., Caporlingua A., Raponi I. et al. Treatment timing and multidisciplinary approach in Apert syndrome. Ann. Stomatol. 2015; 6(2): 58–63.
11.
Fowler P., Hallang S., Snape L. Apert syndrome: an informative long-term dentofacial outcome. BMJ Case Rep. 2022; 15(3): e245224, doi: 10.1136/bcr-2021-245224.
12.
Paes-Souza S.A., Garcia M.A.C., Souza V.H., Morais L.S., Nojima L.I., Nojima M.D.C.G. Response of masticatory muscles to treatment with orthodontic aligners: a preliminary prospective longitudinal study. Dental Press J. Orthod. 2023; 28(1): e232198, doi: 10.1590/2177-6709.28.1.e232198.oar.
13.
Almalki S.A., Al Jameel A.H., Gowdar I.M., Langaliya A., Vaddamanu S.K., Di Blasio M. et al. Impact of clear aligner therapy on masticatory musculature and stomatognathic system: a systematic review conducted according to PRISMA guidelines and the Cochrane handbook for systematic reviews of interventions. BMC Oral Health 2024; 24(1): 350, doi: 10.1186/s12903-024-04029-8.
14.
Horiuchi S., Sato H., Iwasa A., Ichihara A., Tenshin H., Watanabe K. et al. Long-term management of a patient with Apert syndrome. J. Contemp. Dent. Pract. 2021; 22(10): 1184–1190, doi: 10.5005/jp-journals-10024-3201.
15.
Meling T.R., Hans-Erik H., Per S., Due-Tonnessen B.J. Le Fort III distraction osteogenesis in syndromal craniosynostosis. J. Craniofac. Surg. 2006; 17(1): 28–39, doi: 10.1097/01.scs.0000194177.21916.f1.
16.
Johnson D., Wilkie A.O.M. Craniosynostosis. Eur. J. Hum. Genet. 2011; 19(4): 369–376, doi: 10.1038/ejhg.2010.235.
17.
Hohoff A., Joos U., Meyer U., Ehmer U., Stamm T. The spectrum of Apert syndrome: phenotype, particularities in orthodontic treatment, and characteristics of orthognathic surgery. Head Face Med. 2007; 3: 10, doi: 10.1186/1746-160X-3-10.
18.
Raposo-Amaral C.E., Vincenzi-Lemes M., Medeiros M.L., Raposo-Amaral C.A., Ghizoni E. Apert syndrome: neurosurgical outcomes and complications following posterior vault distraction osteogenesis. Childs Nerv. Syst. 2024; 40(8): 2557–2563, doi: 10.1007/s00381-024-06436-2.
19.
Raposo-Amaral C.E., Ghizoni E., Raposo-Amaral C.A. Apert syndrome: selection rationale for midface advancement technique. Adv. Tech. Stand. Neurosurg. 2023; 46: 245–266, doi: 10.1007/978-3-031-28202-7_13.
20.
Wu M., Barnett S.L., Massenburg B.B., Ng J.J., Romeo D.J., Taylor J.A. et al. Early posterior vault distraction osteogenesis changes the syndromic craniosynostosis treatment paradigm: long-term outcomes of a 23-year cohort study. Childs Nerv. Syst. 2024; 40(9): 2811–2823, doi: 10.1007/s00381-024-06465-x.
| eISSN: | 1734-025X |

The Medical University of Silesia in Katowice, as the Operator of the annales.sum.edu.pl website, processes personal data collected when visiting the website. The function of obtaining information about Users and their behavior is carried out by voluntarily entered information in forms, saving cookies in end devices, as well as by collecting web server logs, which are in the possession of the website Operator. Data, including cookies, are used to provide services in accordance with the Privacy policy.
You can consent to the processing of data for these purposes, refuse consent or access more detailed information.
You can consent to the processing of data for these purposes, refuse consent or access more detailed information.