Bieżący numer
Artykuły zaakceptowane
O czasopiśmie
Rada Naukowa
Kolegium Redakcyjne
Polityka prawno-archiwizacyjna
Kodeks etyki publikacyjnej
Wydawca
Informacja o przetwarzaniu danych osobowych w ramach plików cookies oraz subskrypcji newslettera
Archiwum
Dla autorów
Dla recenzentów
Kontakt
Recenzenci
Recenzenci rocznika 2025
Recenzenci rocznika 2024
Recenzenci rocznika 2023
Recenzenci rocznika 2022
Recenzenci rocznika 2021
Recenzenci rocznika 2020
Recenzenci rocznika 2019
Recenzenci rocznika 2018
Recenzenci rocznika 2017
Recenzenci rocznika 2016
Recenzenci rocznika 2015
Recenzenci rocznika 2014
Recenzenci rocznika 2013
Recenzenci rocznika 2012
Polecamy
Śląski Uniwersytet Medyczny w Katowicach
Sklep Wydawnictw SUM
Biblioteka Główna SUM
Polityka prywatności
Deklaracja dostępności
Recenzenci
Recenzenci rocznika 2025
Recenzenci rocznika 2024
Recenzenci rocznika 2023
Recenzenci rocznika 2022
Recenzenci rocznika 2021
Recenzenci rocznika 2020
Recenzenci rocznika 2019
Recenzenci rocznika 2018
Recenzenci rocznika 2017
Recenzenci rocznika 2016
Recenzenci rocznika 2015
Recenzenci rocznika 2014
Recenzenci rocznika 2013
Recenzenci rocznika 2012

Rodzinna jaskra zamkniętego kąta u 48-letniej pacjentki – opis przypadku
1
Students’ Scientific Club at the Department of Ophthalmology, Faculty of Medical Sciences in Katowice, Medical University of Silesia, Katowice, Poland
2
Department of Ophthalmology, Faculty of Medical Sciences in Katowice, Medical University of Silesia, Katowice, Poland
3
Adult Ophthalmology Department, University Clinical Center named after Prof. K. Gibiński, Medical University of Silesia, Katowice, Poland
Zaznaczeni autorzy mieli równy wkład w przygotowanie tego artykułu
Autor do korespondencji
Wiktoria Żelazna
Studenckie Koło Naukowe, Klinika Okulistyki, Wydział Nauk Medycznych w Katowicach ŚUM, ul. Ceglana 35, 40-514 Katowice
Studenckie Koło Naukowe, Klinika Okulistyki, Wydział Nauk Medycznych w Katowicach ŚUM, ul. Ceglana 35, 40-514 Katowice
Ann. Acad. Med. Siles. 2026;80:195-202

SŁOWA KLUCZOWE
DZIEDZINY
STRESZCZENIE
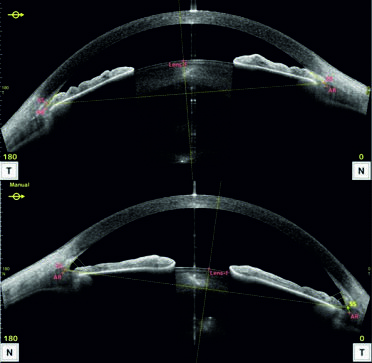
Jaskra pierwotna zamkniętego kąta (primary angle-closure glaucoma – PACG) dotyka ponad 17 milionów ludzi na świecie. Płytka komora przednia i krótka długość osiowa gałki ocznej zwiększają ryzyko zamknięcia kąta przesączania, a w rezultacie rozwoju neuropatii jaskrowej. Rozwój PACG jest także związany z predyspozycją genetyczną. Do poradni okulistycznej zgłosiła się 48-letnia pacjentka. Siostra pacjentki została dwukrotnie poddana witrektomii centralnej odbarczającej z powodu zaawansowanej PACG. Pacjentce zlecono badania dodatkowe: tonometrię, optyczną koherentną tomografię przedniego odcinka oka (anterior segment optical coherence tomography – AS-OCT), gonioskopię i perymetrię statyczną. Pacjentka została zakwalifikowana do profilaktycznej laserowej irydotomii obwodowej (laser peripheral iridotomy – LPI) obu oczu. W badaniach AS-OCT i gonioskopii stwierdzono zamknięty kąt przesączania w oku prawym (oculus dexter – OD), szczelinowaty w oku lewym (oculus sinister – OS) i spłyconą komorę przednią w obu oczach. Ciśnienie wewnątrzgałkowe (intraocular pressure – IOP) wynosiło 20 mmHg w OD i 15 mmHg w OS. Stwierdzono obwodowy ubytek względny pola widzenia w OD. Tonometria kontrolna po 14 miesiącach od wykonania LPI wykazała, że IOP OD wynosi 27 mmHg. Zalecono tymolol 0,5%. Mimo to po 3 miesiącach IOP OD wynosiło 22 mmHg. Pacjentkę zakwalifikowano do powtórnego zabiegu LPI OD. W badaniu kontrolnym IOP OD wynosiło 21 mmHg. Ostrość wzroku wynosiła 1,0 w obu oczach. LPI jest metodą pierwszego rzutu w leczeniu PACG. Mimo wysokiej skuteczności zabieg nie gwarantuje długotrwałego efektu. W razie nawrotu należy rozważyć kwalifikację do zabiegu przeciwjaskrowego.
REFERENCJE (26)
1.
Zhang N, Wang J, Chen B, Li Y, Jiang B. Prevalence of Primary Angle Closure Glaucoma in the Last 20 Years: A Meta-Analysis and Systematic Review. Front Med (Lausanne). 2021;7:624179. doi: 10.3389/fmed.2020.624179.
2.
European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021;105(Suppl 1):1–169. doi: 10.1136/bjophthalmol-2021-egsguidelines.
3.
Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–1911. doi: 10.1001/jama.2014.3192.
4.
Ahram DF, Alward WL, Kuehn MH. The genetic mechanisms of primary angle closure glaucoma. Eye (Lond). 2015;29(10):1251–1259. doi: 10.1038/eye.2015.124.
5.
Shah SN, Zhou S, Sanvicente C, Burkemper B, Apolo G, Li C, et al. Prevalence and Risk Factors of Blindness Among Primary Angle Closure Glaucoma Patients in the United States: An IRIS Registry Analysis. Am J Ophthalmol. 2024;259:131–140. doi: 10.1016/j.ajo.2023.11.007.
6.
Kondkar AA. Updates on Genes and Genetic Mechanisms Implicated in Primary Angle-Closure Glaucoma. Appl Clin Genet. 2021;14:89–112. doi: 10.2147/TACG.S274884.
7.
Wytyczne diagnostyki i leczenia jaskry (aktualizacja 2022). Polskie Towarzystwo Okulistyczne. Warszawa 2022.
8.
Lin Z, Liang Y, Wang N, Li S, Mou D, Fan S, et al. Peripheral anterior synechia reduce extent of angle widening after laser peripheral iridotomy in eyes with primary angle closure. J Glaucoma. 2013;22(5):374–379. doi: 10.1097/IJG.0b013e318241ba1d.
9.
Wright C, Tawfik MA, Waisbourd M, Katz LJ. Primary angle-closure glaucoma: an update. Acta Ophthalmol. 2016;94(3):217–225. doi: 10.1111/aos.12784.
10.
He M, Jiang Y, Huang S, Chang DS, Munoz B, Aung T, et al. Laser peripheral iridotomy for the prevention of angle closure: a single-centre, randomised controlled trial. Lancet. 2019;393(10181):1609–1618. doi: 10.1016/S0140-6736(18)32607-2.
11.
Bao YK, Xu BY, Friedman DS, Cho A, Foster PJ, Jiang Y, et al. Biometric Risk Factors for Angle Closure Progression After Laser Peripheral Iridotomy. JAMA Ophthalmol. 2023;141(6):516–524. doi: 10.1001/jamaophthalmol.2023.0937.
12.
Radhakrishnan S, Chen PP, Junk AK, Nouri-Mahdavi K, Chen TC. Laser Peripheral Iridotomy in Primary Angle Closure: A Report by the American Academy of Ophthalmology. Ophthalmology. 2018;125(7):1110–1120. doi: 10.1016/j.ophtha.2018.01.015.
13.
Azuara-Blanco A, Burr J, Ramsay C, Cooper D, Foster PJ, Friedman DS, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388(10052):1389–1397. doi: 10.1016/S0140-6736(16)30956-4.
14.
Potop V, Corbu C. The role of clear lens extraction in angle closure glaucoma. Rom J Ophthalmol. 2017;61(4):244–248. doi: 10.22336/rjo.2017.44.
15.
Lundström M, Barry P, Henry Y, Rosen P, Stenevi U. Evidence-based guidelines for cataract surgery: guidelines based on data in the European Registry of Quality Outcomes for Cataract and Refractive Surgery database. J Cataract Refract Surg. 2012;38(6):1086–1093. doi: 10.1016/j.jcrs.2012.03.006.
16.
Chen PP, Lin SC, Junk AK, Radhakrishnan S, Singh K, Chen TC. The Effect of Phacoemulsification on Intraocular Pressure in Glaucoma Patients: A Report by the American Academy of Ophthalmology. Ophthalmology. 2015;122(7):1294–1307. doi: 10.1016/j.ophtha.2015.03.021.
17.
Singh K, Aggarwal H, Bhattacharyya M. Phacoemulsification in angle-closure glaucoma: A 360° evaluation. Indian J Ophthalmol. 2024;72(9):1275–1279. doi: 10.4103/IJO.IJO_1701_23.
18.
Kamińska A, Romaniak AM, Izdebska J, Szaflik JP. Surgical lens extraction with vitrectomy in patients with angle-closure glaucoma. Klinika Oczna/Acta Ophthalmologica Polonica. 2021;123(4):218–221. doi: 10.5114/ko.2021.111824.
19.
Noh HJ, Kim ST. Combined treatment of phacoemulsification and single-port limited pars plana vitrectomy in acute angle-closure glaucoma. Int J Ophthalmol. 2019;12(6):974–979. doi: 10.18240/ijo.2019.06.15.
20.
Sachdev R, Gupta A, Narula R, Deshmukh R. Limited vitrectomy in phacomorphic glaucoma. Indian J Ophthalmol. 2017;65(12):1422–1424. doi: 10.4103/ijo.IJO_668_17.
21.
Dada T, Kumar S, Gadia R, Aggarwal A, Gupta V, Sihota R. Sutureless single-port transconjunctival pars plana limited vitrectomy combined with phacoemulsification for management of phacomorphic glaucoma. J Cataract Refract Surg. 2007;33(6): 951–954. doi: 10.1016/j.jcrs.2006.12.037.
22.
Bayliss JM, Ng WS, Waugh N, Azuara-Blanco A. Laser peripheral iridoplasty for chronic angle closure. Cochrane Database Syst Rev. 2021;3(3):CD006746. doi: 10.1002/14651858.CD006746.pub4.
23.
Bourdon H, Aragno V, Baudouin C, Labbé A. Iridoplasty for plateau iris syndrome: a systematic review. BMJ Open Ophthalmol. 2019;4(1):e000340. doi: 10.1136/bmjophth-2019-000340.
24.
Yuasa Y, Sugimoto Y, Hirooka K, Ohkubo S, Higashide T, Sugiyama K, et al. Effectiveness of trabeculectomy with mitomycin C for glaucomatous eyes with low intraocular pressure on treatment eye drops. Acta Ophthalmol. 2020;98(1):e81–e87. doi: 10.1111/aos.14195.
25.
Ye W, Zhang S, Zhu S, Li J, Gu J, Zhao M, et al. 24-month prospective randomized comparison of ab externo penetrating canaloplasty versus trabeculectomy in primary angle-closure glaucoma. Asia Pac J Ophthalmol (Phila). 2025;14(3):100167. doi: 10.1016/j.apjo.2025.100167.
26.
Tham CC, Kwong YY, Baig N, Leung DY, Li FC, Lam DS. Phacoemulsification versus trabeculectomy in medically uncontrolled chronic angle-closure glaucoma without cataract. Ophthalmology. 2013;120(1):62–67. doi: 10.1016/j.ophtha.2012.07.021.
Udostępnij
| eISSN: | 1734-025X |

Śląski Uniwersytet Medyczny w Katowicach, jako Operator Serwisu annales.sum.edu.pl, przetwarza dane osobowe zbierane podczas odwiedzania Serwisu. Realizacja funkcji pozyskiwania informacji o Użytkownikach i ich zachowaniu odbywa się poprzez dobrowolnie wprowadzone w formularzach informacje, zapisywanie w urządzeniach końcowych plików cookies (tzw. ciasteczka), a także poprzez gromadzenie logów serwera www, będącego w posiadaniu Operatora Serwisu. Dane, w tym pliki cookies, wykorzystywane są w celu realizacji usług zgodnie z Polityką prywatności.
Możesz wyrazić zgodę na przetwarzanie danych w tych celach, odmówić zgody lub uzyskać dostęp do bardziej szczegółowych informacji.
Możesz wyrazić zgodę na przetwarzanie danych w tych celach, odmówić zgody lub uzyskać dostęp do bardziej szczegółowych informacji.