Bieżący numer
Artykuły zaakceptowane
O czasopiśmie
Rada Naukowa
Kolegium Redakcyjne
Polityka prawno-archiwizacyjna
Kodeks etyki publikacyjnej
Wydawca
Informacja o przetwarzaniu danych osobowych w ramach plików cookies oraz subskrypcji newslettera
Archiwum
Dla autorów
Dla recenzentów
Kontakt
Recenzenci
Recenzenci rocznika 2025
Recenzenci rocznika 2024
Recenzenci rocznika 2023
Recenzenci rocznika 2022
Recenzenci rocznika 2021
Recenzenci rocznika 2020
Recenzenci rocznika 2019
Recenzenci rocznika 2018
Recenzenci rocznika 2017
Recenzenci rocznika 2016
Recenzenci rocznika 2015
Recenzenci rocznika 2014
Recenzenci rocznika 2013
Recenzenci rocznika 2012
Polecamy
Śląski Uniwersytet Medyczny w Katowicach
Sklep Wydawnictw SUM
Biblioteka Główna SUM
Polityka prywatności
Deklaracja dostępności
Recenzenci
Recenzenci rocznika 2025
Recenzenci rocznika 2024
Recenzenci rocznika 2023
Recenzenci rocznika 2022
Recenzenci rocznika 2021
Recenzenci rocznika 2020
Recenzenci rocznika 2019
Recenzenci rocznika 2018
Recenzenci rocznika 2017
Recenzenci rocznika 2016
Recenzenci rocznika 2015
Recenzenci rocznika 2014
Recenzenci rocznika 2013
Recenzenci rocznika 2012

Analiza parametrów echokardiograficznych wskazujących na nadciśnienie płucne u pacjentów z niewydolnością serca z zachowaną frakcją wyrzutową oraz ocena cech klinicznych sprzyjających rozwojowi fenotypu PH
1
1st Department of Cardiology, Faculty of Medical Sciences in Katowice, Medical University of Silesia, Katowice, Poland; European Reference Network for Rare and Low Prevalence Complex Diseases of the Heart (ERN GUARD-Heart)
Autor do korespondencji
Julia Dołęga
Klinika Kardiologii I Katedry Kardiologii, Śląski Uniwersytet Medyczny w Katowicach, ul. Ziołowa 47, 40-635 Katowice
Klinika Kardiologii I Katedry Kardiologii, Śląski Uniwersytet Medyczny w Katowicach, ul. Ziołowa 47, 40-635 Katowice
Ann. Acad. Med. Siles. 2025;79:92-100

SŁOWA KLUCZOWE
niewydolność sercaniewydolność serca z zachowaną frakcją wyrzutowąpostkapilarne nadciśnienie płucneprzewlekłe migotanie przedsionków
DZIEDZINY
STRESZCZENIE
Wstęp:
Niewydolność serca z zachowaną frakcją wyrzutową (heart failure with preserved ejection fraction – HFpEF) charakteryzuje się dysfunkcją rozkurczową lewej komory (left ventricle – LV). Zaburzenia funkcji rozkurczowej powodują zator płucny i prowadzą do zakapilarnego nadciśnienia płucnego (pulmonary hypertension – PH), które jest istotnym czynnikiem pogorszenia stanu klinicznego i zwiększonej śmiertelności.
Materiał i metody:
Przeprowadzono retrospektywną analizę jednoośrodkową, obejmującą 63 pacjentów hospitalizowanych z powodu HFpEF. Grupę badaną podzielono w zależności od echokardiograficznego prawdopodobieństwa PH na podstawie szczytowej prędkości niedomykalności zastawki trójdzielnej (tricuspid regurgitation velocity – TRV) na dwie grupy: TRV ≥ 2,8 m/s – zwiększone prawdopodobieństwo PH (n = 15 (23,8%); kobiety: 3 (20%); średni wiek 72,7 ± 10,8) oraz TRV < 2,8 m/s – niskie prawdopodobieństwo PH (n = 48 (76,2%); kobiety: 25 (52,1%); średni wiek 72,3 ± 13,7). Przeanalizowano dane kliniczne, parametry echokardiograficzne (transthoracic echocardiography – TTE) oraz wyniki badań laboratoryjnych.
Wyniki:
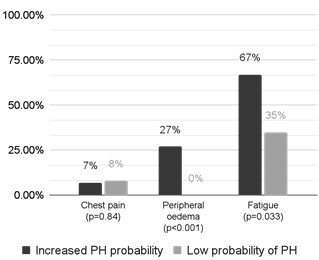
Grupa pacjentów ze zwiększonym prawdopodobieństwem PH cechowała się bardziej nasilonymi objawami HF, częstszym odczuwaniem zmęczenia (p = 0,03) oraz występowaniem obrzęków wokół kostek (p < 0,01). Analiza danych wyjściowych wskazała na tendencję do częstszego migotania przedsionków (atrial fibrillation – AF; p = 0,08) w tej grupie. U pacjentów z TRV ≥ 2,8 m/s obserwowano większą powierzchnię lewego przedsionka (p < 0,001), wyższy wskaźnik E/A (p < 0,001), a także graniczne różnice we wskaźniku masy lewej komory (left ventricular mass index – LVMI; p = 0,06) oraz frakcji wyrzutowej lewej komory (left ventricular ejection fraction – LVEF; p = 0,07).
Wnioski:
U około 25% pacjentów z HFpEF, w większości mężczyzn, występują umiarkowane objawy PH, które wiążą się z bardziej zaawansowaną przebudową i dysfunkcją LV oraz lewego przedsionka (left atrium – LA). Nie znajdują one jednak odzwierciedlenia w typowych chorobach współistniejących, z wyjątkiem AF.
Niewydolność serca z zachowaną frakcją wyrzutową (heart failure with preserved ejection fraction – HFpEF) charakteryzuje się dysfunkcją rozkurczową lewej komory (left ventricle – LV). Zaburzenia funkcji rozkurczowej powodują zator płucny i prowadzą do zakapilarnego nadciśnienia płucnego (pulmonary hypertension – PH), które jest istotnym czynnikiem pogorszenia stanu klinicznego i zwiększonej śmiertelności.
Materiał i metody:
Przeprowadzono retrospektywną analizę jednoośrodkową, obejmującą 63 pacjentów hospitalizowanych z powodu HFpEF. Grupę badaną podzielono w zależności od echokardiograficznego prawdopodobieństwa PH na podstawie szczytowej prędkości niedomykalności zastawki trójdzielnej (tricuspid regurgitation velocity – TRV) na dwie grupy: TRV ≥ 2,8 m/s – zwiększone prawdopodobieństwo PH (n = 15 (23,8%); kobiety: 3 (20%); średni wiek 72,7 ± 10,8) oraz TRV < 2,8 m/s – niskie prawdopodobieństwo PH (n = 48 (76,2%); kobiety: 25 (52,1%); średni wiek 72,3 ± 13,7). Przeanalizowano dane kliniczne, parametry echokardiograficzne (transthoracic echocardiography – TTE) oraz wyniki badań laboratoryjnych.
Wyniki:
Grupa pacjentów ze zwiększonym prawdopodobieństwem PH cechowała się bardziej nasilonymi objawami HF, częstszym odczuwaniem zmęczenia (p = 0,03) oraz występowaniem obrzęków wokół kostek (p < 0,01). Analiza danych wyjściowych wskazała na tendencję do częstszego migotania przedsionków (atrial fibrillation – AF; p = 0,08) w tej grupie. U pacjentów z TRV ≥ 2,8 m/s obserwowano większą powierzchnię lewego przedsionka (p < 0,001), wyższy wskaźnik E/A (p < 0,001), a także graniczne różnice we wskaźniku masy lewej komory (left ventricular mass index – LVMI; p = 0,06) oraz frakcji wyrzutowej lewej komory (left ventricular ejection fraction – LVEF; p = 0,07).
Wnioski:
U około 25% pacjentów z HFpEF, w większości mężczyzn, występują umiarkowane objawy PH, które wiążą się z bardziej zaawansowaną przebudową i dysfunkcją LV oraz lewego przedsionka (left atrium – LA). Nie znajdują one jednak odzwierciedlenia w typowych chorobach współistniejących, z wyjątkiem AF.
REFERENCJE (22)
1.
Eltelbany M., Shah P., deFilippi C. Biomarkers in HFpEF for diagnosis, prognosis, and biological phenotyping. Curr. Heart Fail. Rep. 2022; 19(6): 412–424, doi: 10.1007/s11897-022-00578-7.
2.
Chen Y., Guo H., Xu D., Xu X., Wang H., Hu X. et al. Left ventricular failure produces profound lung remodeling and pulmonary hypertension in mice: heart failure causes severe lung disease. Hypertension 2012; 59(6): 1170–1178, doi: 10.1161/HYPERTENSIONAHA.111.186072.
3.
Karasek D., Sinkiewicz W. Nadciśnienie płucne w przebiegu chorób lewego serca — aktualne leczenie i kierunki rozwoju terapii. Folia Cardiol. 2017; 12(3): 317–325, doi: 10.5603/FC.2017.0061.
4.
Rosenkranz S., Gibbs J.S.R., Wachter R., De Marco T., Vonk-Noordegraaf A., Vachiéry J.L. Left ventricular heart failure and pulmonary hypertension. Eur. Heart J. 2016; 37(12): 942–954, doi: 10.1093/eurheartj/ehv512.
5.
Melenovsky V., Hwang S.J., Lin G., Redfield M.M., Borlaug B.A. Right heart dysfunction in heart failure with preserved ejection fraction. Eur. Heart J. 2014; 35(48): 3452–3462, doi: 10.1093/eurheartj/ehu193.
6.
Humbert M., Kovacs G., Hoeper M.M., Badagliacca R., Berger R.M.F., Brida M. et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022; 43(38): 3618–3731, doi: 10.1093/eurheartj/ehac237. Erratum in: Eur. Heart J. 2023; 44(15): 1312, doi: 10.1093/eurheartj/ehad005.
7.
Corrigendum to: 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: Developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN-LUNG). Eur. Heart J. 2023; 44(15): 1312, doi: 10.1093/eurheartj/ehad005. Erratum for: Eur. Heart J. 2022; 43(38): 3618–3731, doi: 10.1093/eurheartj/ehac237.
8.
Pieske B., Tschöpe C., de Boer R.A., Fraser A.G., Anker S.D., Donal E. et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. Heart J. 2019; 40(40): 3297–3317, doi: 10.1093/eurheartj/ehz641. Erratum in: Eur. Heart J. 2021; 42(13): 1274, doi: 10.1093/eurheartj/ehaa1016.
9.
McDonagh T.A., Metra M., Adamo M., Gardner R.S., Baumbach A., Böhm M. et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2024; 26(1): 5–17, doi: 10.1002/ejhf.3024.
10.
Humbert M., Kovacs G., Hoeper M.M., Badagliacca R., Berger R.M.F., Brida M. et al. Wytyczne ESC/ERS 2022 dotyczące rozpoznawania i leczenia nadciśnienia płucnego. Polskie Towarzystwo Kardiologiczne, 2023-06-13 [online] https://ptkardio.pl/wytyczne/4... [accessed on 3 December 2024].
11.
Hindricks G., Potpara T., Dagres N., Arbelo E., Bax J.J., Blom-ström‑Lundqvist C. et al. Wytyczne ESC 2020 dotyczące diagnostyki i leczenia migotania przedsionków opracowane we współpracy z European Association of Cardio‑Thoracic Surgery (EACTS). Polskie Towarzystwo Kardiologiczne, 2021-03-04 [online] https://ptkardio.pl/resources/... [accessed on 3 December 2024].
12.
Abd-El-Aziz T.A. Noninvasive prediction of left ventricular end-diastolic pressure in patients with coronary artery disease and preserved ejection fraction. Can. J. Cardiol. 2012; 28(1): 80–86, doi: 10.1016/j.cjca.2011.02.001.
13.
Shah A.M., Cikes M., Prasad N., Li G., Getchevski S., Claggett B. et al. Echocardiographic features of patients with heart failure and preserved left ventricular ejection fraction. J. Am. Coll. Cardiol. 2019; 74(23): 2858–2873, doi: 10.1016/j.jacc.2019.09.063.
14.
Shah A.M., Shah S.J., Anand I.S., Sweitzer N.K., O’Meara E., Heitner J.F. et al. Cardiac structure and function in heart failure with preserved ejection fraction: baseline findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist trial. Circ. Heart Fail. 2014; 7(1): 104–115, doi: 10.1161/CIRCHEARTFAILURE.113.000887.
15.
Lam C.S., Roger V.L., Rodeheffer R.J., Borlaug B.A., Enders F.T., Redfield M.M. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J. Am. Coll. Cardiol. 2009; 53(13): 1119–1126, doi: 10.1016/j.jacc.2008.11.051.
16.
Leung C.C., Moondra V., Catherwood E., Andrus B.W. Prevalence and risk factors of pulmonary hypertension in patients with elevated pulmonary venous pressure and preserved ejection fraction. Am. J. Cardiol. 2010; 106(2): 284–286, doi: 10.1016/j.amjcard.2010.02.039.
17.
Obokata M., Reddy Y.N.V., Pislaru S.V., Melenovsky V., Borlaug B.A. Evidence supporting the existence of a distinct obese phenotype of heart failure with preserved ejection fraction. Circulation 2017; 136(1): 6–19, doi: 10.1161/CIRCULATIONAHA.116.026807.
18.
Shah A.M. Ventricular remodeling in heart failure with preserved ejection fraction. Curr. Heart Fail. Rep. 2013; 10(4): 341–349, doi: 10.1007/s11897-013-0166-4.
19.
Santos A.B., Kraigher-Krainer E., Gupta D.K., Claggett B., Zile M.R., Pieske B. et al. Impaired left atrial function in heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2014; 16(10): 1096–1103, doi: 10.1002/ejhf.147.
20.
Freed B.H., Daruwalla V., Cheng J.Y., Aguilar F.G., Beussink L., Choi A. et al. Prognostic utility and clinical significance of cardiac mechanics in heart failure with preserved ejection fraction: importance of left atrial strain. Circ. Cardiovasc. Imaging 2016; 9(3), doi: 10.1161/CIRCIMAGING.115.003754.
21.
Rabkin S.W. Evaluating the adverse outcome of subtypes of heart failure with preserved ejection fraction defined by machine learning: A systematic review focused on defining high risk phenogroups. EXCLI J. 2022; 21: 487–518, doi: 10.17179/excli2021-4572.
22.
Tan Y.T., Wenzelburger F., Lee E., Heatlie G., Leyva F., Patel K. et al. The pathophysiology of heart failure with normal ejection fraction: exercise echocardiography reveals complex abnormalities of both systolic and diastolic ventricular function involving torsion, untwist, and longitudinal motion. J. Am. Coll. Cardiol. 2009; 54(1): 36–46, doi: 10.1016/j.jacc.2009.03.037.
Udostępnij
ARTYKUŁ POWIĄZANY
| eISSN: | 1734-025X |

Śląski Uniwersytet Medyczny w Katowicach, jako Operator Serwisu annales.sum.edu.pl, przetwarza dane osobowe zbierane podczas odwiedzania Serwisu. Realizacja funkcji pozyskiwania informacji o Użytkownikach i ich zachowaniu odbywa się poprzez dobrowolnie wprowadzone w formularzach informacje, zapisywanie w urządzeniach końcowych plików cookies (tzw. ciasteczka), a także poprzez gromadzenie logów serwera www, będącego w posiadaniu Operatora Serwisu. Dane, w tym pliki cookies, wykorzystywane są w celu realizacji usług zgodnie z Polityką prywatności.
Możesz wyrazić zgodę na przetwarzanie danych w tych celach, odmówić zgody lub uzyskać dostęp do bardziej szczegółowych informacji.
Możesz wyrazić zgodę na przetwarzanie danych w tych celach, odmówić zgody lub uzyskać dostęp do bardziej szczegółowych informacji.