Bieżący numer
Artykuły zaakceptowane
O czasopiśmie
Rada Naukowa
Kolegium Redakcyjne
Polityka prawno-archiwizacyjna
Kodeks etyki publikacyjnej
Wydawca
Informacja o przetwarzaniu danych osobowych w ramach plików cookies oraz subskrypcji newslettera
Archiwum
Dla autorów
Dla recenzentów
Kontakt
Recenzenci
Recenzenci rocznika 2025
Recenzenci rocznika 2024
Recenzenci rocznika 2023
Recenzenci rocznika 2022
Recenzenci rocznika 2021
Recenzenci rocznika 2020
Recenzenci rocznika 2019
Recenzenci rocznika 2018
Recenzenci rocznika 2017
Recenzenci rocznika 2016
Recenzenci rocznika 2015
Recenzenci rocznika 2014
Recenzenci rocznika 2013
Recenzenci rocznika 2012
Polecamy
Śląski Uniwersytet Medyczny w Katowicach
Sklep Wydawnictw SUM
Biblioteka Główna SUM
Polityka prywatności
Deklaracja dostępności
Recenzenci
Recenzenci rocznika 2025
Recenzenci rocznika 2024
Recenzenci rocznika 2023
Recenzenci rocznika 2022
Recenzenci rocznika 2021
Recenzenci rocznika 2020
Recenzenci rocznika 2019
Recenzenci rocznika 2018
Recenzenci rocznika 2017
Recenzenci rocznika 2016
Recenzenci rocznika 2015
Recenzenci rocznika 2014
Recenzenci rocznika 2013
Recenzenci rocznika 2012

Czy powinniśmy wykluczyć pacjentów hematoonkologicznych z leczenia otyłości semaglutydem? – opis przypadku
1
Students’ Scientific Club, Department of Internal Medicine and Oncological Chemotherapy,
Faculty of Medical Sciences in Katowice, Medical University of Silesia, Katowice, Poland
2
Department of Internal Medicine and Oncological Chemotherapy, Faculty of Medical Sciences in Katowice, Medical University of Silesia, Katowice, Poland
Autor do korespondencji
Julia Dobrowolska
Studenckie Koło Naukowe, Katedra i Klinika Chorób Wewnętrznych i Chemioterapii Onkologicznej, ul. Reymonta 8, 40-027 Katowice
Studenckie Koło Naukowe, Katedra i Klinika Chorób Wewnętrznych i Chemioterapii Onkologicznej, ul. Reymonta 8, 40-027 Katowice
Ann. Acad. Med. Siles. 2025;79:316-322

SŁOWA KLUCZOWE
DZIEDZINY
STRESZCZENIE
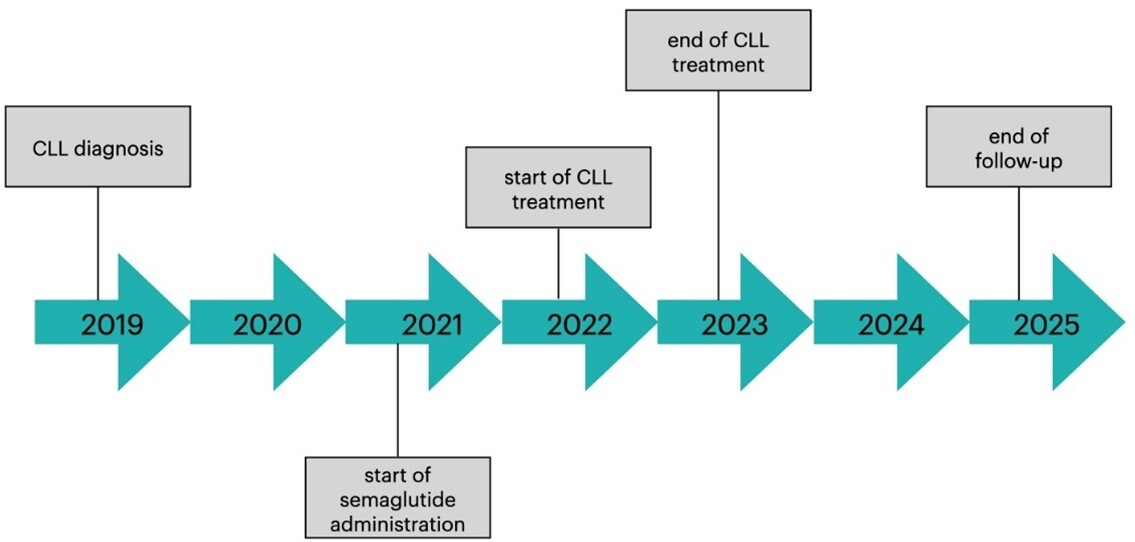
Semaglutyd, będący agonistą receptora glukagonopodobnego peptydu 1 (glucagon-like peptide-1 receptor agonist – GLP-1RA), znajduje szerokie zastosowanie w terapii cukrzycy oraz leczeniu otyłości. Mimo to wciąż brakuje wystarczających danych dotyczących stosowania GLP-1RAs u pacjentów onkologicznych i hematoonkologicznych, ponieważ nie zostali oni uwzględnieni w badaniach klinicznych. Pojawiające się doniesienia o korelacji stosowania GLP-1RAs i nowotworzenia, szczególnie w przypadku nowotworów tarczycy, zrodziło dalsze obawy co do bezpieczeństwa stosowania semaglutydu u pacjentów onkologicznych i hematoonkologicznych. W pracy przedstawiono przypadek 57-letniego pacjenta, chorującego na otyłość III stopnia (BMI: 40,4 kg/m2), cukrzycę typu 2 oraz przewlekłą białaczkę limfocytową (chronic lymphocytic leukemia – CLL; RAI I, Binet A). W celu leczenie otyłości i cukrzycy pacjent rozpoczął terapię semaglutydem, następnie włączono leczenie systemowe CLL obejmujące obinutuzumab z wenetoklaksem; po uzyskaniu remisji CLL kontynuowano leczenie semaglutydem. Ponad 3-letnia terapia semaglutydem pozwoliła na optymalną kontrolę glikemii i spowodowała istotną utratę masy ciała (16% wyjściowej masy ciała pacjenta), podczas leczenia nie odnotowano żadnych działań niepożądanych ani negatywnego wpływu na parametry hematologiczne oraz uzyskaną remisję. Opisany przypadek sugeruje, że pacjentów hematoonkologicznych nie należy kategorycznie wykluczać z leczenia semaglutydem, pod warunkiem zapewnienia właściwego monitorowania parametrów hematologicznych oraz stanu klinicznego. Ponieważ jednak obserwacja opiera się na pojedynczym opisie przypadku, nie można obecnie sformułować jednoznacznych, ogólnych zaleceń dotyczących bezpieczeństwa stosowania semaglutydu w tej grupie pacjentów.
REFERENCJE (26)
1.
Kim D.S., Scherer P.E. Obesity, diabetes, and increased cancer progression. Diabetes Metab. J. 2021; 45(6): 799–812, doi: 10.4093/dmj.2021.0077.
2.
Scully T., Ettela A., LeRoith D., Gallagher E.J. Obesity, type 2 diabetes, and cancer risk. Front. Oncol. 2021; 10: 615375, doi: 10.3389/fonc.2020.615375.
3.
Pasupuleti S.K., Kapur R. The impact of obesity-induced inflammation on clonal hematopoiesis. Curr. Opin. Hematol. 2024; 31(4): 193–198, doi: 10.1097/MOH.0000000000000819.
4.
Zheng Z., Zong Y., Ma Y., Tian Y., Pang Y., Zhang C. et al. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Signal Transduct. Target. Ther. 2024; 9(1): 234, doi: 10.1038/s41392-024-01931-z.
5.
Liu Z.Z., Duan X.X., Yuan M.C., Yu J., Hu X., Han X. et al. Glucagon-like peptide-1 receptor activation by liraglutide promotes breast cancer through NOX4/ROS/VEGF pathway. Life Sci. 2022; 294: 120370, doi: 10.1016/j.lfs.2022.120370.
6.
Mali G., Ahuja V., Dubey K. Glucagon-like peptide-1 analogues and thyroid cancer: An analysis of cases reported in the European pharmacovigilance database. J. Clin. Pharm. Ther. 2021; 46(1): 99–105, doi: 10.1111/jcpt.13259.
7.
Lisco G., De Tullio A., Disoteo O., Piazzolla G., Guastamacchia E., Sabbà C. et al. Glucagon-like peptide 1 receptor agonists and thyroid cancer: is it the time to be concerned? Endocr. Connect. 2023; 12(11): e230257, doi: 10.1530/EC-23-0257.
8.
Piccoli G.F., Mesquita L.A., Stein C., Aziz M., Zoldan M., Degobi N.A. et al. Do GLP-1 receptor agonists increase the risk of breast cancer? A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2021; 106(3): 912–921, doi: 10.1210/clinem/dgaa891.
9.
Smits M.M., Van Raalte D.H. Safety of semaglutide [published correction appears in Front. Endocrinol. 2021; 12: 786732]. Front. Endocrinol. 2021; 12: 645563, doi: 10.3389/fendo.2021.645563.
10.
Piché M.E., Tchernof A., Després J.P. Obesity phenotypes, diabetes, and cardiovascular diseases [published correction appears in Circ. Res. 2020; 127(3): e107, doi: 10.1161/RES.0000000000000421]. Circ. Res. 2020; 126(11): 1477–1500, doi: 10.1161/CIRCRESAHA.120.316101.
11.
Avgerinos K.I., Spyrou N., Mantzoros C.S., Dalamaga M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019; 92: 121–135, doi: 10.1016/j.metabol.2018.11.001.
12.
Lichtman M.A. Obesity and the risk for a hematological malignancy: leukemia, lymphoma, or myeloma. Oncologist 2010; 15(10): 1083–1101, doi: 10.1634/theoncologist.2010-0206.
13.
Aoyagi T., Terracina K.P., Raza A., Matsubara H., Takabe K. Cancer cachexia, mechanism and treatment. World J. Gastrointest. Oncol. 2015; 7(4): 17–29, doi: 10.4251/wjgo.v7.i4.17.
14.
Bruggeman A.R., Kamal A.H., LeBlanc T.W., Ma J.D., Baracos V.E., Roeland E.J. Cancer cachexia: beyond weight loss. J. Oncol. Pract. 2016; 12(11): 1163–1171, doi: 10.1200/JOP.2016.016832.
15.
Ligibel J.A., Bohlke K., May A.M., Clinton S.K., Demark-Wahnefried W., Gilchrist S.C. et al. Exercise, diet, and weight management during cancer treatment: ASCO guideline. J. Clin. Oncol. 2022; 40(22): 2491–2507, doi: 10.1200/JCO.22.00687.
16.
O’Connell F., O’Sullivan J. Help or hindrance: The obesity paradox in cancer treatment response. Cancer Lett. 2021; 522: 269–280, doi: 10.1016/j.canlet.2021.09.021.
17.
Assumpção J.A.F., Pasquarelli-do-Nascimento G., Duarte M.S.V., Bonamino M.H., Magalhães K.G. The ambiguous role of obesity in oncology by promoting cancer but boosting antitumor immunotherapy. J. Biomed. Sci. 2022; 29(1): 12, doi: 10.1186/s12929-022-00796-0.
18.
Cleto A.S., Schirlo J.M., Beltrame M., Gomes V.H.O., Acras I.H., Neiverth G.S. et al. Semaglutide effects on safety and cardiovascular outcomes in patients with overweight or obesity: a systematic review and meta-analysis. Int. J. Obes. 2025; 49(1): 21–30, doi: 10.1038/s41366-024-01646-9.
19.
Colin I.M., Gérard K.M. Once-weekly 2.4 mg semaglutide for weight management in obesity: a game changer? touchREV. Endocrinol. 2022; 18(1): 35–42, doi: 10.17925/EE.2022.18.1.35.
20.
Bezin J., Gouverneur A., Pénichon M., Mathieu C., Garrel R., Hillaire-Buys D. et al. GLP-1 receptor agonists and the risk of thyroid cancer. Diabetes Care 2023; 46(2): 384–390, doi: 10.2337/dc22-1148.
21.
Meeting highlights from the Pharmacovigilance Risk Assessment Committee (PRAC) 23-26 October 2023. European Medicines Agency, 27 October 2023 [online] https://www.ema.europa.eu/en/n... [accessed on 12 April 2024].
22.
Feier C.V.I., Vonica R.C., Faur A.M., Streinu D.R., Muntean C. Assessment of thyroid carcinogenic risk and safety profile of GLP1-RA semaglutide (ozempic) therapy for diabetes mellitus and obesity: A systematic literature review. Int. J. Mol. Sci. 2024; 25(8): 4346, doi: 10.3390/ijms25084346.
23.
Nagendra L., Bg H., Sharma M., Dutta D. Semaglutide and cancer: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2023; 17(9): 102834, doi:10.1016/j.dsx.2023.102834.
24.
Ashruf O.S., Hundal J., Mushtaq A., Kaelber D.C., Anwer F., Singh A. Hematologic cancers among patients with type 2 diabetes prescribed GLP-1 receptor agonists. JAMA Netw. Open 2025; 8(3): e250802, doi: 10.1001/jamanetworkopen.2025.0802.
25.
Sørum M.E., Gang A.O., Tholstrup D.M., Gudbrandsdottir S., Kissow H., Kornblit B. et al. Semaglutide treatment for PRevention Of Toxicity in high-dosE Chemotherapy with autologous haematopoietic stem-cell Transplantation (PROTECT): study protocol for a randomised, double-blind, placebo-controlled, investigator-initiated study. BMJ Open 2024; 14(10): e089862, doi: 10.1136/bmjopen-2024-089862.
26.
Vainer N., Rotbain Curovic V., Niemann C.U., Slager S.L., Rotbain E.C. Understanding the interplay between chronic lymphocytic leukemia and type 2 diabetes. Expert Rev. Hematol. 2024; 17(9): 617–629, doi: 10.1080/17474086.2024.2383417.
Udostępnij
ARTYKUŁ POWIĄZANY
| eISSN: | 1734-025X |

Śląski Uniwersytet Medyczny w Katowicach, jako Operator Serwisu annales.sum.edu.pl, przetwarza dane osobowe zbierane podczas odwiedzania Serwisu. Realizacja funkcji pozyskiwania informacji o Użytkownikach i ich zachowaniu odbywa się poprzez dobrowolnie wprowadzone w formularzach informacje, zapisywanie w urządzeniach końcowych plików cookies (tzw. ciasteczka), a także poprzez gromadzenie logów serwera www, będącego w posiadaniu Operatora Serwisu. Dane, w tym pliki cookies, wykorzystywane są w celu realizacji usług zgodnie z Polityką prywatności.
Możesz wyrazić zgodę na przetwarzanie danych w tych celach, odmówić zgody lub uzyskać dostęp do bardziej szczegółowych informacji.
Możesz wyrazić zgodę na przetwarzanie danych w tych celach, odmówić zgody lub uzyskać dostęp do bardziej szczegółowych informacji.